
SHARP Awards for Health IT Establish Web Sites
Web sites have been launched for each of the four advanced research projects announced April 2, 2010 by the Office of the National Coordinator (ONC) for Health IT. The program called Strategic Healthcare IT Advanced Research Projects (SHARP), totalling $60 million over four years, taps into four consortia of leading reseach and academic institutions each led by a major research institution. “The research projects supported by the SHARP program will focus on solving current and expected future challenges that represent barriers to adoption and meaningful use of health IT. These projects will focus on areas where ‘breakthrough’ advances are needed to realize the full potential of health IT.” This chart was taken from the Mayo Clinic College of Medicine Wiki site for its project.

- SHARP Organization
1. Security of Health IT
http://sharps.org
University of Illinois at Urbana-Champaign
Strategic Healthcare IT Advanced Research Projects on Security (SHARPS)
SHARPS is accociated with the Center for Health Information Privacy and Security in the Information Trust Institute at the University of Illinois at Urbana-Champaign
In their research overview, SHARPS describes the structure of their project, “SHARPS is organized around three major environments: Electronic Health Records (EHRs), Health Information Exchanges (HIEs), and Telemedicine (TEL), with Personal Health Records (PHRs) included as a major subtopic. SHARPS research projects in these strategic areas are interconnected through three cross-cutting themes: conceptual and policy foundations, service models, and open validation.”
People
Research
Jobs
Publications
Links
2. Patient-Centered Congnitive Support
http://sharpc.org
The University of Texas Health Science Center at Houston
National Center for Cognitive Informatics and Decision Making in Healthcare (NCCD)
Alternative URL: http://www.uthouston.edu/nccd
Mission: “The mission of the NCCD is to bring together a collaborative, interdisciplinary team of researchers from across the nation; with the highest level of expertise in patient-centered cognitive support research from biomedical and health informatics, cognitive science, clinical sciences, industrial and systems engineering, and health services research. Additionally, the NCCD will conduct short-term research that addresses the urgent usability , workflow, and cognitive support issues of Health Information Technology ( HIT) as well as long-term, breakthrough research that can fundamentally remove the key cognitive barriers to HIT adoption and meaningful use. The center will translate research findings to the real world through a cooperative program involving researchers, patients, providers, HIT vendors, and other stakeholders.”
Projects |
Project Title |
|
| Project 1 | Work-Centered Design of Care Process Improvements in HIT | |
| Project 2A | Cognitive Foundations for Decision Making: Implications for Decision Support | |
| Project 2B | Modeling of Setting-Specific Factors to Enhance Clinical Decision Support Adaptation | |
| Project 3 | Automated Model-based Clinical Summarization of Key Patient Data | |
| Project 4 | Cognitive Information Design and Visualization: Enhancing Accessibility and Understanding of Patient Data | |
| Project 5 | Improving Communication in Distributed Team Environment |
3. Health Application and Network Platform Architectures
http://www.smartplatforms.org
Harvard University
Substitutable Medical Apps, reusable technologies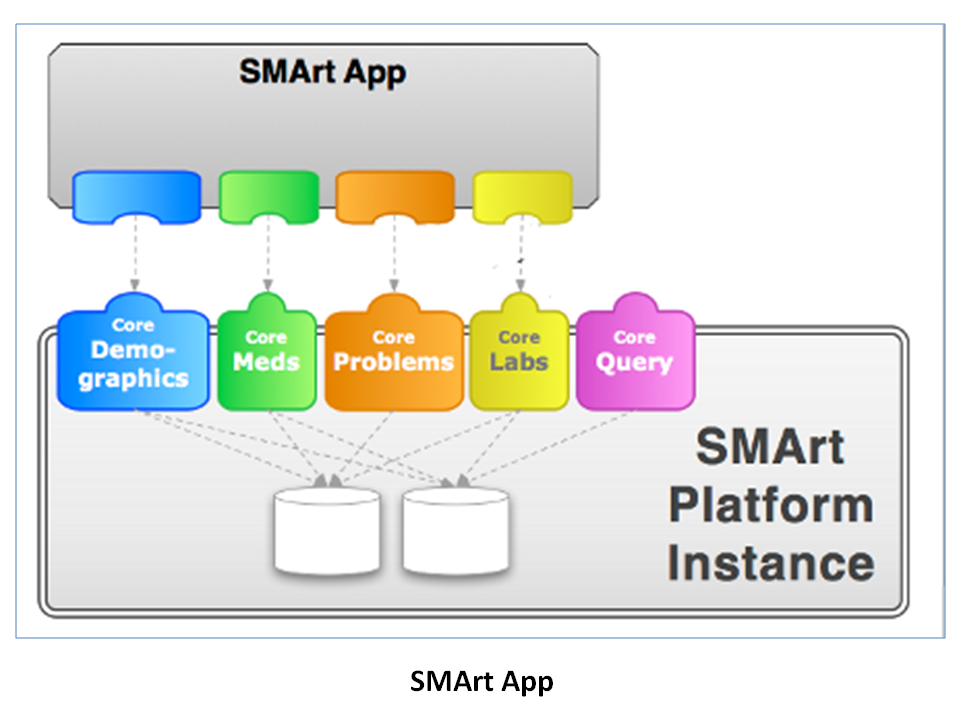
The March 26, 2009 essay by Kenneth D. Mandl, MD, MPH, and Isaac S. Kohane, MD, PhD, in New England Journal of Medicine “No Small Change for the Health Information Economy”. They wrote “A health care system adapting to the effects of an aging population, growing expenditures, and a diminishing primary care workforce needs the support of a flexible information infrastructure that facilitates innovation in wellness, health care, and public health.” They reference the flexbility of applications and the stable platform provided by the iPhone.
PDF: http://content.nejm.org/cgi/reprint/360/13/1278.pdf
Ten principles were developed at a subsuquent workshop setup on May 13, 2009 by the”Informatics Program at Children’s Hospital Boston (CHIP) “of leading experts in health, innovation and technology to define ten core principles of a platform that would support healthcare information technology.” See “Ten Principles for Fostering Development of an ‘iPhone-like’ Platform for Healthcare Information Technology”
4. Secondary Use of EHR Data
http://sharpn.org
Mayo Clinic College of Medicine
Per Mayo Clinic College of Medicine Wiki: “We propose research that will generate a framework of open-source services that can be dynamically configured to transform EHR data into standards-conforming, comparable information suitable for large-scale analyses, inferencing, and integration of disparate health data. We will apply these services to phenotype recognition (disease, risk factor, eligibility, or adverse event) in medical centers and population-based settings. Finally, we will examine data quality and repair strategies with real-world evaluations of their behavior in Clinical and Translational Science Awards (CTSAs), health information exchanges (HIEs), and National Health Information Network (NHIN) connections.
“We have assembled a federated informatics research community committed to open-source resources that can industrially scale to address barriers to the broad-based, facile, and ethical use of EHR data for secondary purposes. We will collaborate to create, evaluate, and refine informatics artifacts that advance the capacity to efficiently leverage EHR data to improve care, generate new knowledge, and address population needs. Our goal is to make these artifacts available to the community of secondary EHR data users, manifest as open-source tools, services, and scalable software. In addition, we have partnered with industry developers who can make these resources available with commercial deployment. We propose to assemble modular services and agents from existing open-source software to improve the utilization of EHR data for a spectrum of use-cases and focus on three themes: Normalization, Phenotypes, and Data Quality/Evaluation. Our six projects span one or more of these themes, though together constitute a coherent ensemble of related research and development. Finally, these services will have open-source deployments as well as commercially supported implementations.
“There are six strongly intertwined, mutually dependent projects, including: 1) Semantic and Syntactic Normalization; 2) Natural Language Processing (NLP); 3) Phenotype Applications; 4) Performance Optimization; 5) Data Quality Metrics; and 6) Evaluation Frameworks. The first two projects align with our Data Normalization theme, while Phenotype Applications and Performance Optimization span themes 1 and 2 (Normalization and Phenotyping); while the last two projects correspond to our third theme.”
SHARP Program Organization
SHARP Area 4: Themes & Projects
Project Initiation Meeting Slides PDF
For more recent post about SHARP Program on e-Healthcare Marketing, click here.

